Heuristics are rules of thumb used by experts. Part 1 of this study described their nature, the changed context of surgical dissection in the past two centuries and its mechanical basis
This second part is the core of this study, aimed directly at the practising surgeon, the teacher, and the trainee. It describes practical rules for dissection and controlling accuracy of hand movement which fall into several convenient groups. The first two groups, dividing and gripping, relate most to tissue properties, and the other two, controlling and timing, mostly relate to the operator. They are listed in Table 1.
1. Cut at right angles to lines of tension
Prodding or stroking limp tissue does not progress the course of a dissection. Such repeated ineffective movements are characteristic of a novice but also seen with experienced operators (apart from when they are testing or confirming the strength of tissue to avoid an "oops!"). Lines of tension must be established at right angles to the proposed incision and this can be done in several ways.
1. Pulling a structure anchored at one end by the weight of the body
or by tension of a retractor
2. Pulling apart two points, each held in fingers, forceps, by tape, gauze,
retractors, transfixed by suture or other ways. A special case is the
use of one type of the double hand-grips used by surgeons (Fig. 1a).
Fig. 1 Double hand-grip for tensing tissue 
3. Tensing a structure by distending it from within, squeezing it at
the back while it remains tethered or pushing it from behind. Unlike the
previous two methods, the lines of tension are curved rather than in a
straight line, and they may radiate in several directions rather than
being parallel.
4. Relying on quick movement and the inertia of the target
Tension in a stretched structure can be increased by pulling it over a convexity, such as a finger, in the third method just listed. Applying a double hand-grip to small bowel and its adjoining mesentery allows well-controlled safer sharp or blunt dissection of the peritoneum and fat. An added advantage in this activity is that bleeding from an accidentally torn vessel can be controlled with just a little extra tension by wrapping the mesentery more snugly over the fingers by lifting it slightly. This heuristic is not available to the laparoscopic operator unless a hand-assisted technique is used.
Tissue which is under intrinsic tension will part in a pleasing way with light strokes of a scalpel (Fig 1b) though the margin for error and cutting the inner surface becomes small.
Fig. 2 Tissue parting under intrinsic tension![]()
An example is dividing the outer coats of a benign cyst such as a hydrocoele. A blunt instrument such as a probe can also divide tense tissue, for example a congenital pyloric tumour, once the initial sharp cut has been made. In the latter case the underlying gastric mucosa fall away with a modest margin of safety except at the dangerous duodenal fornix where the mucosa is infolded and more firmly attached.
A structure is best divided parallel to its grain, for example a muscle-splitting incision. The strength of its main fibres is greater than the finer fibrils holding them together, and healing of this connective tissue is more effective than of cut larger structures. Rubbing away loose tissue which is hiding a structure for better visibility uses a similar principle on a smaller scale, for example gauze on a pledget or wrapped over a finger, catching small fibres and stretching and tearing them.. Even a toothbrush can be used to define Calot's triangle in a laparoscopic cholecystectomy but why stop at laparoscopic procedures to use brushes of various types or suitably ended fine rakes?
Finger fracture, coarse squeezing of a crumbly structure, works well on a crumbly solid organ such as liver, with the added advantage of not dividing firmer structures such as blood vessels (even delicate veins, with care) and ducts as readily as parenchyma. Occasionally it is useful for separating peritoneal adhesions if they are weaker than the loops of bowel or other vital structures they stick together.
To tear elastic or plastic tissue, , especially when view is limited,
apply the two graspers next to each other before pulling them apart (Fig
2). 
Fig.3 Two graspers put next to each other before tearing tissue. If they are two far apart, the tissue won't tear but just spring back
Pulling on tissue which is elastic or plastic will not tear it until its limits for these properties are exceeded - by definition. (As mentioned in Part 1, a tentative weaker pull may be needed to test or confirm the strength of the tissue) In laparoscopic surgery there is only a limited cone of view, about 60 degrees across, compared with 120 degrees for the two eyes normally. (Sharp macular vision is of course much more limited in extent, about 2 degrees across). The physical space for manoeuvre is also restricted, though compared with a small abdominal incision the distended abdominal cavity gives a much roomier view, for example in an appendicectomy in an obese patient.
In this limited area of view, if the two graspers are not placed close
together no tearing will occur before they move out of the limited area
of view, perhaps bumping against other structures or damaging them.
This also concentrates force between the two instruments being pulled
over a narrower cross-section, increasing the effectiveness of the applied
force - the old principle of divide and conquer.
Obvious as this might be, it applies also to dividing tissue by scratching at it. If the tissue is limp, it just moves with each push or pull, instead of separating, and just flops back into place. To dissect tissue in this way, its surface layer must be made taut. If there are projecting fronds of tissue, such as on fatty omentum, each one must be pulled away from the line of dissection to one side or the other, perhaps by the friction of gauze, like long hair on the head which is parted, pulled by the friction of the overlying hand, and then tied snugly on each side. Repeated ineffective prodding is commonly seen at operation and on video replays, failing to advance the progress of the operation.
The mechanism of dividing by scratching is like the slicing action of a blade described earlier. The difference in this case is that instead of many tiny teeth, the end of the dissector is a single tooth, gaining a purchase on the tissue which varies with the direction of application, its shape, and the coarseness of the fibrous structure of the tissue.
3. Push and indent to grasp a flat surface
To grasp a flat surface of tissue facing the instrument, push its open jaws in to create two dints, and therefore an intervening ridge (Fig. 3).
Fig. 4 Deforming tissue provides a protrusion
There are two sequences shown here.
The first is Grip > Slip > Oops > Grip > etc
The second one shows pushing down harder with the jaws open
This creates two indentations. The protrusion between them can now be gripped.
The mechanics of grasping tissue in laparoscopic surgery have been analysed previously . The heuristic not considered at that time deals with deforming tissue to provide a protrusion or flange to fit between jaws.
Grasping onto a flat surface is a typical laparoscopic scenario because mobility of instruments is restricted to four degrees of freedom (roll, pitch, yaw, z-axis) with no x-axis or y-axis movement if the port site is not moved by stretching. They are also quite limited in range except for the in-out movement along the z-axis. Finding an edge to grasp is difficult.
A typical repeated sequence of ineffective movements by the novice is Grip > Slip > Oops > Grip > etc. The forceps fail to grip the structure because no part of it is between the jaws as they are being closed..
The heuristic of the expert is to move more slowly and in particular to begin by pushing down with the opened jaws onto the surface (Fig 7), not so forcefully as to break through it if damage to deeper structures is a concern.
Provided the structure or what underlies it is supple enough, this creates two indentations (Fig 8), with a ridge formed between them. It will not work with smooth ended forceps pressing onto a smooth hard surface, such as a mesh for repairing an inguinal hernia when it is resting on the pubis. Fine teeth at the jaw tips might just manage to catch fine fibres of the material and create a fold as the jaws are closed
If the pushing continues as the jaws of the forceps are closed, the protruding tissue between them is compressed and deformed by ridging inside the jaws so it will not slip out. Grasping the tissue is then successful and the tissue can be pulled on or drawn to one side or the other.
This model of successful grasping of tissue by using indentation is plausible
and supported by video clips of surgery showing this phenomenon. (Fig
3b)
Fig. 5 Frame from a video clip of surgery. It shows the jaws of an open grasper pressing onto stomach.
Below it is an explanatory sketch
4.. Increase accuracy of movement with a fulcrum
Use a support to steady the hand and fingers and instruments. Controlling the accuracy of hand movement is a concern in all areas of surgery. It is worse in abdominal endosurgery because the hands while gripping the end of long instruments, lack steadying support, and because of the wide excursions of the working end relative to movement of the hands. This is aggravated if the shoulders are held abducted in a "chicken-wing" position (discussed below).
The problem of controlling fine movement or normal hand tremor in microsurgery was solved 25 years ago . Of a dozen factors influencing the amplitude of tremor, the most effective is how close the support is for the hand or instrument to the point of engagement with the work being done. The further away, the greater the amplitude of unwanted movement (Fig 4a).
Fig.6 Tremor and point of limb support (after Voigt )
The ultimate example of using this principle is drawing a straight line with a ruler.
In laparoscopic surgery this is the distance between the instrument tip and the fulcrum where the shaft passes through a cannula in the abdominal wall, unless there is support other than the fulcrum. Such support might be resting the shaft of the instrument against an intra-abdominal structure, or a mechanical device outside the abdomen. The forearm or upper arm may be steadied against the body or against another member of the operating team, or the operator's fingers may rest on the port cannula (Fig 4b).
Fig. 7 Steadying the fingers on the skin of the forearm for greater steadiness during cannulation of a vein
The last kind of support is difficult or not possible for a device with finger controls such as a diathermy or a sucker rather than a foot control. One of the unstated advantages of hand-assisted laparoscopic surgery may be that the intra-abdominal hand and fingers are supported against viscera within the abdomen, and can in turn steady the tissues and instruments being manipulated.
An extreme example of lack of support is the "chicken-wing" or scarecrow-like posture of a laparoscopic operator holding the arms outwards instead of supported against the sides of the trunk (Fig 4c)
Fig. 8 Chicken-wing posture
This occurs when the hands have to be held too high. The wrist flexion also limits mobility and control of hand grip. This is determined by several factors - the relative height of the table, height of the operator (or assistant), any platform they may be standing on, the length of instruments within and outside the abdomen, the placement of port sites, and obesity of the patient. .
Standing on a platform to overcome this problem may cause on its own problems - hitting one's head against the overhead light, and having a foot control which slithers about and falls off the platform, unless it has a small barrier around it, especially at the edge. Some upwards tilt of the patient away from the operator (feet down for the upper abdomen and feet up for the pelvis) favours better posture for the operator as well as a falling away of viscera from the operating area which would otherwise obscure it. The common problem of operating tables not lowering far enough is well-recognised, but like the weather, nobody seems to do anything about it.
When using lever-like support a further example is shortening the effective distance by providing a fulcrum near the target. This is the basis for controlling hand movement by providing support, mentioned above. Where Archimedes said he could move the earth if he had a long enough lever and a fulcrum to rest it on, the micro-surgeon might claim to be able to move a single atom, given enough visual information and a fulcrum sufficiently close. Indeed one of the advantages of laparoscopic surgery is the greater clarity of detail possible because of how close the lens can be positioned to the target. The advent of such "precision surgery" was predicted in the 1970s .
The common type of example, shortening the unsupported distance by supporting the hand or fingers in microsurgery, is seen in examples such as watchmaking, threading a needle while steadying the hands against each other, putting a needle into a needleholder (Fig 4d),
Fig. 9 Putting a needle into a needleholder. The tips of the fingers are steadied against the needleholder, held out at arms-length by someone else.
or even more powerfully by using a ruler to draw a straight line. Most effective of all is eliminating human hand-grip from the loop by automating the task and using sufficiently steady machinery. One step short of this is using computer-mediated movement to scale it down by a high factor, and this is currently one of the selling points for semi-robotic systems for microsurgery.
(A Cartesian robotic arm has to be bulky and heavy if it is to be steady. A system of three converging arms can be made much lighter and steadier, but needs much more powerful computers than are currently practical to calculate the polar co-ordinates quickly enough ).
5. Fitts' law - make target bigger and closer
Fitts' Law is a very robust law in psychology. It states that the time it takes to touch a target depends on how far away it is, and how wide, confirming everyday experience and intuition. The closer and larger a target, the quicker you can reach it accurately. Its formal statement is:
t = a + b * log 2 * d / w
where
t = time taken to reach target
a & b are constants
d = distance to target
w = width of target
This has numerous examples. On a computer screen, the larger a button, the more accurately and quickly the cursor can be placed over it by moving the mouse. A mechanical model is inserting a peg in a hole (Fig 5).
Fig. 10 Peg and hole, showing Fitts' Principle
If they have exactly the same diameter, this is practically impossible. If the peg is tapered, and the hole is widened at its entrance, the effective diameter of the target is increased dramatically. If it is too sharp, the point will catch on irregularities or penetrate a soft object - a matter of judging the balance between too blunt and too sharp.
Apart from tapering and chamfering, this equation can be manipulated in practice by increasing the apparent diameter of the target, for example by using magnification, or increasing visual acuity by improving lighting, colour contrast or other factors. Under magnification, a small insect in a spider's web looks like a soccer ball in a goal and can be manipulated much more easily.
6. Extending the Fitts Principle - control the direction of movement using the Funnelling Principle
Use a funnel to guide movement. A funnel serves to constrict a widely scattered range of trajectories of moving objects to a narrower one. Funnels are generally thought of for liquids but they apply to solid objects as well. The sides provide a constraint or mechanical barrier to movement beyond it, just as a ruler constrains otherwise shaky movement of a hand-held pencil to a straight line, extending the one-dimensional heuristic of using a ruler to three dimensions. There are two-dimensional examples such as moving a mob of sheep between converging fences so they form a single line to enter the dipping trough one at a time, or merging traffic lanes, or constraining the movements of a ball in a pin-ball machine.
Here are a few surgical instances:
" Fitting together mechanical connections of many kinds: Examples are tapered syringe nozzles and needle hubs, tubing connectors, and fitting the head of a bed onto the end of the bed. Sometimes these are too short to grasp properly, like a shortened endotracheal tube, violating an ergonomic principle of design for handling.
" Intubating hollow structures: A vein is generally distended with a tourniquet to make it a bigger target, while other hollow structures could be but aren't.
" Inserting a T-tube into a common bile duct: Here the problem is getting the two short arms of the T-junction through a slit, either by clumsy stretching or by tucking the second half of the cross-tube under the first part - easier said than done for some operators.
" Cannulating the cystic duct with a round-ended plastic tube: This is a formidable challenge if the cystic duct is narrow. Conversely, if a stylet is too sharp or rigid it will catch on the lining of the duct.
" Controlling the direction of movement: The first step is achieving some alignment of the two structures to be mated, before the mechanics of the design take fine control over from the operator's body.
" Entering an acute angle instead of working away at an obtuse angle - entering a narrow angle to separate two structures where they are converging. Separating a muscle with an oblique fleshy attachment from bone (e.g. external intercostal muscle from rib) is far better done working into the acute angle between them rather than the opposite way, into the obtuse angle when the muscle will tear. The enjoyable Irish anatomist A K Henry calls this the stripping angle (Fig. 6a)
Fig. 11 The stripping angle between the external intercostal muscle and the upper border of a rib. You strip forwards along the upper border, and backwards along the lower border
and gives many examples of using it in his landmark book, sadly unfamiliar to many of today's practising surgeons and teachers and to those in training. A related example is when separating the gall-bladder from the under surface of the liver, dividing at the angle of peritoneal attachment or the areolar tissue in the bed. It is all too common to have an unintended perforation of the gall-bladder, spilling bile and stones with delay to the procedure and possible complications.
" Separating structures which have been fused by fibrotic scar: The simple rule is to start where the tissues have not been involved, separate them there, and work round the circumference of a circle at each deeper layer to reach vital structures at risk of damage. Common examples are the exploration of recurrent or persisting sapheno-femoral incompetence, recurrent hernias, and inflammation and scarring about the cystic duct.
This same funneling angle can also be used for another heuristic, picking the direction of pull to give the smallest and therefore weakest cross-section of attachment to pull on. When building nests, ravens strip twiglets in the one direction, away from the acute angle, to concentrate leverage on the smallest possible target of fibers under tension (Fig 6b).
Fig. 12 Raven stripping twiglets
When separating two planes by traction (see above) less force is needed along a narrow edge rather than a broad edge, with the added bonus of less error and easier correction.
7. Control the limit to movement
Unlike the swing of a racquet or polo stick or the arm in throwing, movements in surgery are nearly all incremental rather than ballistic. The common exception is a jab or shove for penetrating a layer in one movement as in suturing or cannulating a vessel once the point of the needle is engaged in position just into the surface of the structure.
To avoid unwanted effects where the range of tolerance for error is small, such movements require exceptional judgment and skill, or else a mechanical barrier to prevent overshoot or an "oops!" experience. A large scale example is the buffer at the end of a railway line. A small-scale example is controlling the depth of an intramuscular injection by positioning the wrist so that the ulnar edge of the hand hits the skin when the needle is at the desired depth (Fig.7)
Fig. 13 Buffering the extent of a ballistic movement, so you and the patient don't have an oops! experience.
In a thin patient this avoids the embarrassing clunk of the needle tip hitting bone. It applies to controlling movement of a diathermy hook so it does not damage adjoining structures such as liver or bowel.
Unintended little burns are common on the under surface of the liver at laparoscopic cholecystectomy. It is important to increase the margin of safety for such movements, by increasing the separation of structures, by taking smaller bites, or having a safety layer or shield.
Eli Whitney, the inventor of the cotton gin, was a New England engineer
and inventor who made his fortune in the 1800s manufacturing flintlock
guns to be used in wars against the French and their native Indian allies.
In 1797 he popularised mass production, as described by Daniel Bell .
He wanted to transfer his skills to the workers he employed, so he devised
a series of jigs and measures to be used to ensure the accuracy of sizes
of the different components they made for him to a higher degree of accuracy
than they could achieve by eye on their own. This had the great advantage
of making parts interchangeable instead of hand-fitting each gun as the
individual product of a master craftsman.
The common use of templates, stencils and outlines for tracing are examples
of the same principle. In surgery, they are used to lay out measurements
in cosmetic procedures on the breast or for complicated skin flaps. Such
mechanical guides and measuring tools are part of a more general rule,
discussed earlier and again in the next heuristic.
8. ecrease the amplitude of tremor of the hand and body
The problem of tremor in microsurgery was introduced earlier in describing the value of a fulcrum for steadiness. Everyone has hand tremor and other unwanted body movements. In the outstretched fingertips, it has an amplitude of a half to three millimetres and an irregular frequency of 7 to 30 vibrations per second. It is affected by about a dozen factors, discussed previously in relation to microsurgery. The same factors that control tremor also allow more accurate control of fine movement.
Support is the single most immediate and effective factor. Sign-writers and oil-painters use a padded "maulstick" to rest the painting hand on without smudging their work like using a ruler to draw a straight line (Fig. 8a).
Fig. 14 Maulstick anti-tremor support
A laparoscopic diathermy stick can be steadied against the port, provided it does not have finger-controls on it which need manipulation (Fig. 8b).
Fig. 15 Steadying a laparoscopic diathermy. This is traced from a picture of my colleague Dr. Luis Isabel at work.
Even with the greater part of the length of the instrument within the
abdomen there is much finer control than the usual uncontrolled 1 - 3
mm excursion of the tip. (One surgeon interviewed in a related study using
a think-aloud protocol considered that control was best when half the
shaft length of the instrument was within the abdomen, which does not
accord with the geometry of the situation).
Surgeons can support their body by sitting, leaning against the operating
table or resting their arms on it or the patient, which sometimes interferes
with the patient's breathing or equipment such as tubing. They may need
better designed instruments so their hand-grips allow good standing posture.
At times less experienced laparoscopic operators have their arms out like
chicken-wings, as described earlier.
9. Avoid excess force and muscle tension
Using excessive force increases the amplitude of hand tremor 5. Such excess force may take three forms. One is pushing too hard, on an instrument for example, a second is gripping it too hard, shown in handwriting by a white-knuckle grip and hyperextension of the distal interphalangeal joint of the index finger (Fig. 9)
|
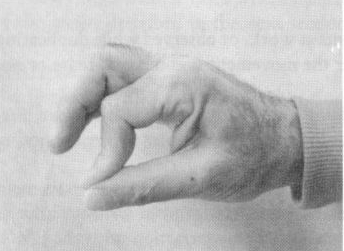
Fig. 16 White-knuckle grip of pen from unnecessarily foreful grip.
and a third is excessive simultaneous contraction of agonist and antagonist muscles 13, 14 . A physically tense surgeon is less skilful than might be otherwise, like musicians, sportspersons, and other workers.
Such muscle tension is sometimes forced on the operator by stiff instruments such as forceps and needleholders . Many of the microsurgical needleholders available in 1970 required a 10 Newton handgrip to close their jaws, instead of the optimal 0.6 - 0.9 N. Just to grip a needle with a laparoscopic needleholder requires a tense grip because of the poor needle-holding ability of most instruments available
10. Use good timing to tear accurately along tissue planes
Good timing is necessary for separating cleanly along a tissue plane
by tearing. It is a feature of many different types of skilled activities.
Often it is easy to recognise but hard to define without some further
analysis. Consider pushing a child on a swing. If the push is at the correct
phase of the swing, it does not need to be a strong one, and it can be
repeated with only a little effort each time to give a big build up of
energy. If applied at the wrong phase of the swing there is a jarring
effect, wasting energy. In such a case the definition of good timing is
"that rate of application of force which maximises the transfer of
energy."
It applies to a hammer or an axe ("Let the hammer do the work"),
a golf swing, a karate chop, or lifting a bag of wheat onto a truck. A
skilled railway construction worker hitting a tie with a sledgehammer
uses its recoil as the start of the backswing instead of wasting this
energy.
Such "ballistic" timing was referred to earlier 1 when it was noted to have little part in surgical dissection, when skilful movement is incremental, a little at a time.
Separating tissue cleanly along an anatomical plane by pulling to each side must be done slowly enough for successive groups of fibrils to stretch and disrupt. Pulling more quickly means that one or other side may be weaker than the cohort of connecting fibres, and tearing will occur through it instead.
This can be demonstrated by splitting an ordinary business card. Start a split at one corner and pull the two layers apart slowly (Fig. 10).
Fig. 17 Splitting a business card
If you hold the card close to your ear you can hear five or ten crackles
a second. Look at the business card you are splitting under magnification,
for example an operating microscope at medium power. You will see fibres
of different sizes tearing at a similar rate to the crackles heard earlier.
Individual fibres appear to take a finite time to stretch before they
tear. If torn apart too quickly, the combined strength of several cohorts
of fibres prove stronger than either of the split sheets, which tear so
the plane is lost. Slower is quicker. Observations from existing surgical
videos as well as common experience should confirm this.
Other tissue aspects of timing
Squeezing tissue quickly disrupts it. When the wall of small intestine is compressed gently by clamps or forceps, it takes minutes rather than seconds to displace extra-cellular fluid so it diffuses under the pressure through the interstices of the tissue .
Presumably like the timing to split tissue cleanly it takes time for fluid to percolate through a fine mesh or gel, and a quicker application will cause fractures of the tissue elements. Older studies on the effect of stiff vascular clamps showed later atheroma development , while small vessels showed disruption of the intima from microvascular clamps but these did not consider the rate of application of force, or how sharp or rounded the edges of the clamp jaws were. Presumably there was no special slowing of the process of clamping the vessels.
There are many common examples of the importance of timing such as cooking, the setting of plaster or cement, hitting a tennis ball and how quickly to decide diagnosis or action in a surgical emergency without errors of hast
e. Physical, chemical and biological processes all take time to complete. A computer doesn't fire up in an instant though a calculator may appear to.
11. Take time to look and think
Thinking takes time. It takes time for ideas to "sink in", through as yet mysterious mental processes, but governed by elements of time based on formation of new glial fibres and synapses (at a probable rate of a million each second unlike the old traditional static view of brain structure), action potentials, travel across synapses, summation and so on. In the human brain a typical sequence of sensation processing response takes 80 - 100 milliseconds for each phase, in total a third of a second for the immediate response to some simple event (Fig 11)
Fig 18 It takes time for a loaf of bread to rise, and for an idea to gel
Please a cartoon of bread, and time for thought bubble to illuminate light bulb
Typically an expert takes longer to look at and assess a situation because a novice perceives much less and compares sensations and perceptions with a much smaller mental library of stored visual and other images. Once the expert gets going, of course, things happen with fewer and smaller delays and mistakes.
12. Pre-position to make the next move easier
Take time for an extra movement early in a sequence to save extra avoidable moves later. Events in a procedure do not proceed in a simple linear fashion. Sometimes there is a branch in the sequence. The following example is from suturing rather than dissecting but shows the issue clearly. When a suture needle has been passed through tissue, the next step may not be to pick it up again, but to grasp the suture elsewhere to form a knot. If the needle is put down "anywhere", it may be difficult to find or to pick up again, particularly if the view is limited in extent, in micro or lap surgery. Further, if visibility is poor, it may be camouflaged against the background. Inadvertent traction on the suture may flick the needle further away, further out of sight.
Fig. 19 Setting up time includes motor and peerceptual preparatory activities
Pleaseimagine a cartoon of a golfer getting into position,practising swing, feet shuffling, and head looking down and ahead several times.
A structure or the end of a suture must be placed where it can avoid being shifted, be seen clearly and then grasped successfully. In microsurgery the tiny needle may be placed secure from accidental movement in a temporary position by sticking its point into muscle or other firm tissue near the edge of the field of view. The operator needs to create and place a loop of the suture to sit nearby without tangling, and so it can be easily seen and grasped by the needleholder for creating a knot. Both should be put on tissue which contrasts with them, which is difficult with a dark suture and dark background. Similarly a coloured plastic strip is often placed behind a microsurgical anastomosis to make the ends of the structures and the suture more easily visible.
Another help for this is in a suitable design of suture, perhaps a contrasting green or medium blue, or with an alternating colour of segments every few millimetres or contrasting strands to heighten its visibility, of which commercial examples are just starting to appear. Both the needle and the suture should be placed so they are not stuck flat by moisture to the surface making it difficult to grasp them, perhaps by inserting just the point of the needle.
One way of pre-positioning a needle easily is to use an alternating grip needleholder, which is now commercially available.for endo-suturing. Such a device was described by Tibbs several decades ago for use in open surgery but never became popular. In such a mechanism the needle is always secured by one or both of the two pairs of jaws, like the shuttle in a textile machine.
Dissecting analogues for pre-positioning were discussed at the beginning - setting up lines of tension. Others include positioning tissue, or oneself, for better visibility or for a better-controlled direction of movement. In the case of the famous gastrectomist, WJ Ferguson, referred to in Part 1, I was able to tell whether he was dissecting the lesser curve or the greater curve from the position of his feet, glimpsed past the hinge of the door to his operating theatre. It was as predictable as the stance of a good tennis player making an unhurried forehand or backhand stroke.
Learning heuristics does not eliminate the need for repetition to make a skill automatic and subconscious and to establish good timing, but it may shorten the learning curve in two ways - selecting the best of several possible movements, and making it explicit. The only heuristic that appears to gain mention in the literature is tension. Power writes "In praise of tension", pointing out that tissues are normally tightly packed in the body and must be disentangled for view. Other uses he describes include tissue division, retraction, and controlling bleeding but he describes the dangers of distortion dragging structures into unsafe positions or making a large vein look like a strand of connective tissue. Kirk illustrates several different ways of applying tension and its value in displaying a tissue plane to dissect along.
Reasons for improving operative skills and their teaching were discussed in Part 1 of this study. At a basic skills workshop on suturing and tying of knots one finds interns inept in these skills, where those of an earlier generation keen on a surgical career would practice tying knots on the bedpost during their literally named residency. Teaching basic skills like this does not come easily if based only on personal experience of the task. Today's computers, CDs and methods of analysis described above should make these tasks much easier, though not as a total substitute for the human teacher.
Studies, textbooks and handbooks on surgical technique describe stitching and knotting in detail, some in a masterly way, like the text by Szabo and Berci . However it is typical that such texts do not consider the heuristics of dissection. Nor does dissection yet figure heavily in workshops for trainee surgeons, except perhaps for cutting out a circle or star of rubber glove or pig skin.
Materials for suturing are easy to provide and don't need a lot of cleaning up afterwards. Performance is easier to measure and describe. Perhaps it is like the old story of the drunk looking for his car-keys under the lamp-post instead of the car-park, "because the light is better there" .
There is a need to develop heuristics further, to validate them, to devise models for workshop teaching, and to include them in the basic training of surgeons. Detailed task analyses of the type used here may explain the violent differences of opinion about many alternative types of procedure, for example laparoscopic repair of inguinal hernia, and the reasons why they appear much easier for some operators than others.
Two kinds of knowledge - declarative and procedural
Psychologists have long recognised that there are two kinds of memory, termed declarative and procedural . These adjectives are also applied to two kinds of knowledge. Declarative knowledge is what is "declared" or taught formally. This is the shared knowledge of textbooks. Procedural knowledge is the knowledge of "how", and includes skills like riding a bicycle or - dissecting! - learned like the tune of a song rather than the words The two are considered by neuroscientists as quite different, remembered and forgotten by different mechanisms, and perhaps learned in different ways. Perhaps the first kind is more accurately labelled information, giving a useful though far from clean division of properties (Table 2)
Procedural knowledge seems to correspond closely to heuristics described in this study. Perhaps the transformation of implicit into explicit knowledge by the descriptions provided here suddenly provides a short circuit between the two, between what is implicit and unspoken and what is explicit and shared formally. If so, the implications go far beyond a few rules for surgical dissection.
In Part 1 we discussed the three stages of history of surgery as Pre-Modern,
Modern, and Post-Modern. Perhaps the future will see the emergence of
an additional Fourth Age of Autonomous Surgery carried out by robots.
In this the human input in real-time will be limited to nominating the
terms of each sub-task or series of tasks at their beginning, starting
them, letting this automated procedure run, and use its results for further
steps or procedures. The scenario, mediated by mouse, graphics tablet,
or voice recognition might run something like:
" Move mouse to starting point of incision,
" left click,
" move to end point,
" click to define and display line of incision,
" right click,
" select dissecting mode from drop-down menu - scalpel, diathermy,
ultrasound, laser …. ,
" select or modify preset input values for patient's tissue diathesis,
tissue thickness, detailed pathology, specific boundary values and over-riding
events …. ,
" left click to confirm …."
Or the operator might say, "the heck with it. Close Robot. Open manual mode please".
While such an era of automated surgery does not concern us directly here, the design of these tasks of the future will also need an understanding of current manual expertise and skilled perception and movement in surgery, even though their method of implementation will be different. In industry this scenario exists in the construction of expert systems (see below).
The costs of studying and teaching heuristics are minimal compared with other areas of surgery. Discovering them is a matter of individual interest, or study of existing operative videotapes on a standard personal computer. Teaching them in principle is a barely measurable cost, and material for training workshops should be relatively cheap. The crucial, invisible and uncosted element is the intelligence applied by the teacher. The cost-benefits of applying heuristics have already been mentioned.
Their importance for planning robotic surgery has also been mentioned. Of course it is unlikely that a simulacrum of the hand will be part of such systems, being replaced by more simply and efficiently engineered substitutes. However the lessons to be carried over are those of the sensitivity and pliability of fingertips and the placement, grading and timing of applied forces. Haptics, the study of touch and tactile sensations, is a significant part of future systems, extended to recognition of shapes and other properties of objects such as consistency and weight. Artificial vision, smell, and sound may also be part of this new sensory equipment, and extended far beyond the normal human spectra of sensitivity and perception.
Such blue-skies thinking may be decades into the future, but whatever practice exists then will need a convergence both of these concepts and the technology to come. For the immediate needs of surgery now and the near future the clear need is for more effective manual surgical technique based in part on a new approach of heuristics, based on a realisation of its importance and the support of surgeons..
References
(see end of Part 1)
-o0o-
Contents
1. Cut at right angles to lines of tension
2. Tear, don't just stretch
3. Push and indent to grasp a flat surface
4. Increase accuracy of movement with a fulcrum
5. Fitts' law - make target bigger and closer
6. Extending the Fitts Principle - control the direction of movement using the Funnelling Principle
7. Control the extent of movement
8. Control tremor of the hand and body
9. Avoid excess force and muscle tension
10. Good timing and tearing along tissue planes
11. Take time to look and think
12. Pre-position to make the next move easier