During a surgical operation, it is good to decrease the amount of physical work done by the surgeon, for several reasons. If much force is needed to pierce tissues during suturing, these are more likely to tear; if the surgeon has to press harder, he has less accurate control of the needle; exertion aggravates the normal physiological tremor, impairing fine manipulation; simple fatigue has a detrimental effect.
Avoidable heavy work by the surgeon may be due to many factors, including poor posture, heavy pull on tissue (particularly if badly designed instrument handles are used), excessive force needed to close the ratchets of artery forceps and needleholders, and lack of sharpness in suture needles. The last two factors will be discussed in this paper.
Force necessary to lock artery forceps
The quality of artery forceps and needleholders is reflected in the stiffness or lack of temper of the handles, and is assessed partly by the force necessary to engage or release the ratchet. This force can be measured by a simple method (Patkin, 1969). The instrument is supported lightly by one hand, so that handle movement would he In the vertical plane. The handles are then compressed on to a kitchen scale, by the other hand (Figure 1).
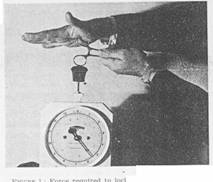 Figure 1: Force required to lock first step of ratchet
Figure 1: Force required to lock first step of ratchet
Many surgeons will be surprised to know that there is a recommended range of force for closing the first step of the ratchet on a pair of Spencer‑Wells artery forceps. The British Standard Specification (B.S. 3355:1961) reads as follows:
"7. The pressure required to be applied on the bows to close the forceps on the first step of the rack shall be between 3 lb and 4 1/2 lb (1.36 and 2.04 kg). "
In practice, this recommendation is often ignored. One such instrument tested personally required 9 lb (about 4 kg) to close the first notch, twice that force to close the second notch, and even more squeeze in the same direction, or a lateral push of 3 lb (1.4 kg) to disengage the ratchet. This equipment bears the stamp of a major supplier of surgical equipment and is a recent model with a box joint.
Such heavy forces needed for disengagement may give the assistant great difficulty and sometimes tear off an important and inaccessible vascular pedicle such as an awkward mesoappendlx. When surgeons come across a stiff instrument of this type, they may find it more effective than simple comment to communicate to the instrument curator the force necessary to work a particular instrument.
More important, an occasional but regular cheek in this way on forceps making up a laparotomy set will weed out defective equipment before it is presented to the surgeon d during an operation, and a certain amount of bloodshed or adverse comment may be avoided. This aspect of instrument quality should also be taken into account d during the purchase of artery forceps.
Force necessary to lock needleholders
With a good quality Hegar needleholder, the force necessary to close the first, second and third notches may be 2.6 kg, 3.2 kg and 3.8 kg respectively. With a merely average quality Matthews needleholder, the force necessary for closure may be over 9 lb, (4 kg), incompatible with good suturing, even though closure is effected by the mechanically better‑placed thenar eminence.
A personally designed needleholder, based on analysts of the “internal precision grip" of the hand (Patkin, 1969) does away with the need for a locking mechanism. The strength of grip necessary to stop a needle twisting about depends on tissue resistance (tissue nature and needle point), needle shaft design, jaw Inserts (such as copper or tungsten carbide), and mechanical advantage (low with Gillies' needleholder).
Microsurgical needleholders
The discrepancies in locking force for these expensive instruments are even wider. Four new needleholders were assessed at a recent weekend workshop in microsurgery held at the Royal Alexandra Hospital for Children, Camperdown. The force necessary for engagement of the ratchet varied from 150 gm with a Catford pattern, to over 1200 gm with one example of a Castroviejo needleholder. The force in the latter case seems excessive when only 50 gm may be necessary for piercing a 2 mm artery with a 5/0 atraumatic suture, and little extra force is needed to tear the tissue, which may occur as the needleholder is being unlocked If the operator's posture is a difficult one.
The expert microsurgeon finds he does best with such an Instrument by removing the ratchet altogether (Earl Owen, personal communication). This is easily done on a workshop bench. Some microsurgeons have approached the problem by devising a remote‑control foot‑pedal mechanism for opening and closing the jaws; Salmon (1968) described a pneumatic system, and Acland (1969) devised a hydraulic system. Other possibilities are a mechanical system using Bowden cable, or electrical systems using a high‑voltage solenoid or a micrometer and reduction gear. Such remote control systems lack simplicity. One solution is a mini-version of the writer's ergonomically designed needleholder (Patkin, 1969).
Tissue resistance to needle penetration
Nurses and doctors, as well as patients, know how much apparently similar needles can vary in the force necessary to penetrate human tissue. A kitchen scale used for measuring handle stillness will also show the force necessary for penetrating tissue by a needle.
In this technique, a patch of tissue removed at operation, such as skin from a mastectomy specimen, opened out artery, or a strip of aponeurosis, is pinned out over a perforated support such as a cotton reel. The needle to be tested may be straightened If appropriate, and held either In the hand or a needleholder. The amount of force exerted when penetration occurs is readily seen on the scale (Figure 2). The reading taken is the highest figure during slow passage or the needle, as one cannot measure the true force when the momentum of a "shove" is used, a frequent and Important component of suturing technique technique which minimizes tissue trauma In many sites.

FIGURE 2 : Force required to penetrate tissue.
A sample of skin or other tissue is pinned to the side of a cotton reel over the hole and the needle pushed through the tissuer sample.
A more elaborate method used a Chatillon gauge instead of a five-dollar guage.
As an example, resistance of previously scarred linea alba to a hand needle ranges between five and ten pounds' weight. This may force the occasional hand ‑stitcher to revert to the use of a needleholder, especially if he uses smooth rubber gloves rather than the finely mammillated ones recommended by Tanner (personal communication) or cotton overgloves (Hughes, 1968). The forces that a surgeon can exert on a needle can be measured In the same way, pressing directly on to the scale.
Surgeons would find it useful for surgical needle makers and instrument curators to assess needle sharpness quantitatively by means of an inexpensive synthetic standard.
References
Acland R. D. (1969), "Modified Needleholder for Microsurgery", Brit. med. J., 1: 635.
British Standards Institution (1961), "Spencer Wells Artery Forceps (Straight and Curved) with Box Joints, British Standard 3355.
Hughes, E S R and Moynihan, B, (1968), "Cotton Overgloves”, Med J.Aust 1 : 220.
Patkin, M. (1969), "Ergonomic Design of a Needleholder ‑, Med. J. Aust., 2: 490.
Salmon, P. A. (1968), "A New Technique of Microsuture for Blood ‑Vessel Anastomosis", Brit. J. Surg., 55: 58.
-o0o-
Summary
Physical effort during surgical operations is discussed, especially the force necessary to close instruments provided with a ratchet, and the resistance of tough tissues to penetration by a needle. Better selection and checking of surgical equipment for quality are recommended.
___________________
Surgical instruments and effort referring especially to ratchets and needle sharpness
January 31,1970 The Medical Journal of Australia pps 225-226
Shorter Communications
Michael Patkin, MBBS FRCS FRCSEd FRACS. D ungog, N SW
Dr M. Patkin, "Cangon", Dungog, NSW 2420. Honorary Medical Officer, Dungog and District Hospital .
_______________
Thirty five years later, I see mention of the Matthew needle-holders ( and ) which would be unknown to surgeons today, while the Hegar needle-holder was the ordinary ring=handled type.
The whole idea of measuring forces at surgery is still an unusual one, though not as much today.
I applied the same idea to measuring tenderness.