TENDERNESS is one of the few signs of clinical medicine which is not measured or recorded in terms of number. It is described using adjectives, in such terms as very slight, mild, moderate, marked, and exquisite. Although the same pathological process gives tenderness which varies from one individual patient to another, some importance is attached to its absolute level. In some situations, such as deciding whether to operate upon patients with peritonitis or possible intraabdominal bleeding, great reliance is placed on a change in the level of tenderness.
For such reasons, it would seem useful to attempt to measure tenderness in terms of the amount of force, applied gradually, that it takes to cause pain to the patienl.
In an ordinary, spring operated kitchen weighing scale, the pan is replaced by a long bolt and some rubber disks carrying a large rubber knob, actually a rounded tip for a chair leg, measuring 4cm in diameter (Figure 1).
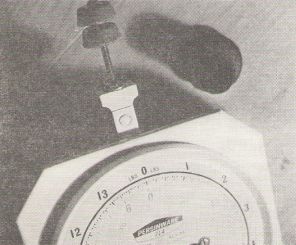
This "tenderness meter" can be put together in a hardware shop in a few minutes. The scale setting must be adjusted so that a zero reading is shown with the instrument upside down and the rubber tip just starting to exert downward pressure on a horizontal surface.
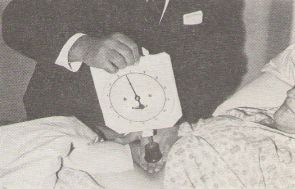
In actual use, the instrument is held upside down by one hand. Its weight is gradually allowed to be taken up by that part of the abdomen or other part of the patient's body being tested, and pressure is gradually applied over a period of 10 or 20 seconds (Figure 2).

The patient is asked to say when he feels pain as a result of the increasing
pressure in such terms as "tell me as soon as you feel it just starting
to hurt".
When this occurs, the reading on the scale is noted, at what might be
usefully, if crudely, termed the "ouch point".An alternative
method of use (Figure 3) is to place one hand nil the patient's abdomen in the normal posture
for palpation. and to apply the knob of the tenderness meter to the backs
of the fingers so that its force is transmitted passively.
The latter method allows more than just the visual appreciation of muscle guarding. No difference has been noted in the measurements obtained by the two methods.
Case 1. A plump man, aged 30 years, had a two day history of appendicitis, confirmed later at operation. He had tenderness on pressure of 31/2 lb weight (1,600 gm) at McBurney's point. The further away from this point on the abdominal wall, the greater the force required to elicit tenderness (Figure 4).
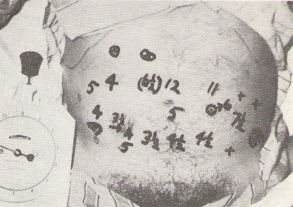
Repeated measurements showed some alterations, which remained stable on a third examination. This could be attributed to a shift of bowel and inflammatory exudate, similar to that invoked to explain the mechanism of Rovsing's sign.
Case 2. A boy, aged nine years, was admitted to hospital at Dungog after a fall from a horse, during which his abdomen was hurt. Initial examination showed no more than slight tenderness in the left hypochodrium on manual palpation. Between two and two and a half hours after admission, his pulse rate rose from 100 to 120 beats per minute. On account of a rare accident, telephone communication from sister to doctor broke down temporarily. On her own initiative, the sister made use of the tenderness meter. which happened to be. within the hospital. She noted maximum tenderness to be under the left hypochondrium elicited by a pressure of 2 lb 12 oz (1,250 gm). Thirty minutes later, it took only 2 lb (900 gm) to elicit the same tenderness (Table 1).
TABLE 1
Measurements of tenderness and pulse rate (Case, 2)
| Hours after admission | Pulse Rate(Beats per Minute) | Minimum Force to Elicit Pain |
|
0
|
92
|
|
|
0.5
|
98
|
|
|
1
|
100
|
|
|
1.5
|
98
|
|
|
2
|
100
|
|
|
2.5
|
120
|
|
|
3
|
116
|
|
|
3 . 5
|
122
|
2 lb 12 oz(1,250 gm)
|
|
4
|
120
|
2 lb (900 gm)
|
|
4.5
|
115
|
Transfer to theatre
|
At operation a little later, between 200 and 300 ml of intra-peritoneal blood was found, and a ruptured but otherwise normal spleen was excised. Daily postoperative measurements of tenderness showed an interesting and gradual reversion to normality, in accord with common sense experience (Figure 5),

splenectorny (Case 2).
Measurements on a number of other patients showed that marked or "acute" tenderness corresponded to a pressure of 1 lb to 2 lb (500 to 1,000gm, approximately), moderate tenderness to a pressure of 4 to 5 lb (about 2,000 gm), and slight tenderness to a pressure of 6 to 8 lb (3,000 to 4,000 gm). Tenderness of a skin boil was elicited with pressures of only a few grammes.
These personal levels were found to correspond closely to those of several surgical colleagues, who were asked to apply pressure corresponding to what they considered to be mild, moderate, or marked tenderness. Presurnably these figures agreed because of proprioceptive impulses learned by doctors from a common pool of patients and symptoms.
Discussion
This brief experience hints at the possible value of a simple and cheap instrument which can be used to measure tenderness. It may be of help in making earlier decisions in such conditions as diverticulitis not responding sufficiently well to conservative treatment, a retroperitoneal tear of the duodenum not declaring itself clearly, or peritoneal irritation from other causes. Objective trials in a busier surgical centre than Dungog would be needed to form any reliable opinion on this possibility.
The apparatus can be used hy a trained nursing sister, in the absence
of a doctor, much as if the pulse or the
temperature was being measured. It may be used when the care of a patient
is transferred from one doctor to another many miles away, or when a patient
is far from medical help, as on a ship at sea or in a space craft.
The "tenderness meter" described is cumbersome, and hardly likely to be carried like a stethoscope in the pocket or a thermometer in the bag. There are compact engineering instruments the size of a large pencil, known as "push pull" gauges, which can measure the same range of force, and which would be much more convenient. Their price, unfortunately, is 10 times that of the kitchen scale illustrated
I am grateful to Sister Margaret Smith (now Mrs R. Jones, of Dungog), who demonstrated so effectively that measurement of tenderness by a trained nurse was perfectly feasible, and who used her initiative to such good effect. I remain deeply indebted to Dr Henry Smith, of Morpeth, who travelled far over country roads to administer a perfect anaesthetic to the patient described in Case 2.
-o0o-
Contents
TechniqueClinical experience
Discussion
Acknowledgements
____________
Measurement of tenderness
with the description of a simple instrument
A method is described for the measurement of tenderness, instead of using adjectives to indicate its level. Brief clinical experience and implications for further study are discussed.
The Medical Journal of Australia March 28, 1970, p670
Reprinted in Pain - Clinical and Experimental Perspectives, Ed. Wiesenberg (Mosby, St. Louis).
__________________
Michael Patkin MBBS.(MELB.), FRCS(Eng), FRCS(EDIN.), FRACS
1 Honorary Medical officer.
Address for reprints: Dr M. Patkin, Cangon, Dungog, N.S.W.
Dungog and District IIospital, New South Wales
________________
One factor to control, not specified in the original paper, is the rate of application of force.
Most people are not used to judging forces numerically. Exceptions are clerks in post offices and sellers of fruit by weight. They have repeated feedback during the working day of the weights of letters, packages, or pieces of fruitso they learn from experience what 200 grams or a kilgram feel like.
Sir Francis Galton, a brilliant scholar, correlated the ability to judge forces with the hand with intelligence.
See elsewhere [q.v.] my spectrum of forces exerted in everyday life.